
As for all the other congenital bleeding disorders, replacement therapy is currently the only effective management option for FVII deficiency2,20,24 and is the main treatment for spontaneous bleeds, severe cases, surgical hemostasis, and for individuals with a bleeding history.37 Factor replacement therapy may also be used for prophylaxis in children with severe FVII deficiency.38
Besides plasma-derived FVII concentrates, other potential therapies for management of FVII deficiency include fresh frozen plasma (FFP), 4-factor prothrombin complex concentrates (PCCs), and recombinant FVIIa (rFVIIa). The latter is the only treatment supported by substantial research studies and is considered the first-line treatment option, if available.2,21,25
Treatment of FVII deficiency is characterized by the short in vivo half-life of FVII, low FVII recovery, and rapid FVII clearance, which is more evident in children.39 Because of these features, replacement regimens require frequent dosing.
FFP and PCCs were widely used in the past, but the risk of circulatory overload and the simultaneous administration of clotting factors other than FVII limit their use, primarily because of the risk of thrombotic complications.40 Plasma-derived concentrates of FVII (Provertin UM TIM3; 600 IU per 10 mL; Baxter) are effective at doses of 30–40 U/kg.40 The risk of blood-borne pathogen transmission with this product, although theoretically possible, is extremely low because of viral inactivation procedures.
Recombinant activated FVII (rFVIIa; Novoseven®; Novo Nordisk) is the most widely accepted therapeutic option for inherited FVII deficiency, both for spontaneous bleeding and in surgical settings.2,21,22 The recommended dosage of 15-30 µg/kg q4-6h is used to maintain FVII levels above 15%-20%.19,41,42,43
A new formulation of rFVIIa that is stable up to 25 ˚C has been tested in a randomized, double-blind trial that assessed equivalence with the original formulation in terms of safety, efficacy and pharmacokinetic parameters.44 Differences did exist in the determination of rFVIIa plasma levels, especially very low levels, when different assays were used.43 Repeated average doses of 20 µg/kg have been reported in a number of papers from the Seven Treatment Evaluation Registry (STER) to be effective in achieving hemostasis, but optimal treatment regimens have not been defined.29,30,37,38
Asymptomatic patients undergoing minimally invasive surgery, such as dental procedures, can be successfully treated with tranexamic acid given both orally or intravenously at the usual dosages.
Figure 4 shows a summary of the factor concentrates that are used for the treatment of FVII deficiency.
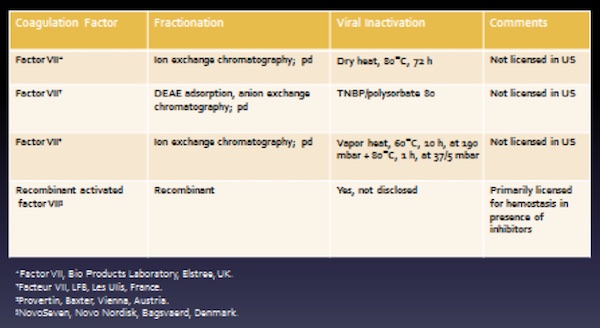
Adapted from Mannucci PM, et al. Blood. 2004;104:1243-1252.
