
The FVIIc assay is readily available, but the results can be influenced by the different thromboplastins used in the specific assay. In addition, tiny residual amounts of FVII present in the assay may reduce assay sensitivity, a consideration that is particularly important for the diagnosis of qualitative defects such as FVII Padua. The use of a standardized reference plasma as a calibrator and a recombinant thromboplastin as a common reagent have reduced the variability of inter-laboratory assays, particularly when determining low to very low levels of plasma FVIIc.32,33
Molecular diagnosis of FVII deficiency is based on conventional PCR techniques. Given the poor relationship between FVIIc and the bleeding tendency, molecular diagnosis is helpful in unsolved cases or in cases in which the inheritance pattern in not clear. More complex intragenic re-arrangements that are not detected by conventional PCR-based techniques can be identified by semi-quantitative multiplex PCR. This approach can provide a full mutational status in individuals with FVII deficiency.9
Prenatal diagnosis should be proposed only if a family history of severe bleeding is present. Cord blood is usually obtained by either the trans-abdominal or trans-amniotic approach. Genetic analysis of blood samples is the gold standard method for prenatal diagnosis. Given that FVII deficiency is very rare, mutational gene analysis may not be available. For such cases, an FVIIc assay obtained by cordocentesis between the 17th and 21st weeks of gestation is feasible, but reconfirmation is needed after birth.34.35 Alternatively, prenatal diagnosis can be performed by amniocentesis during the early stage of pregnancy.36
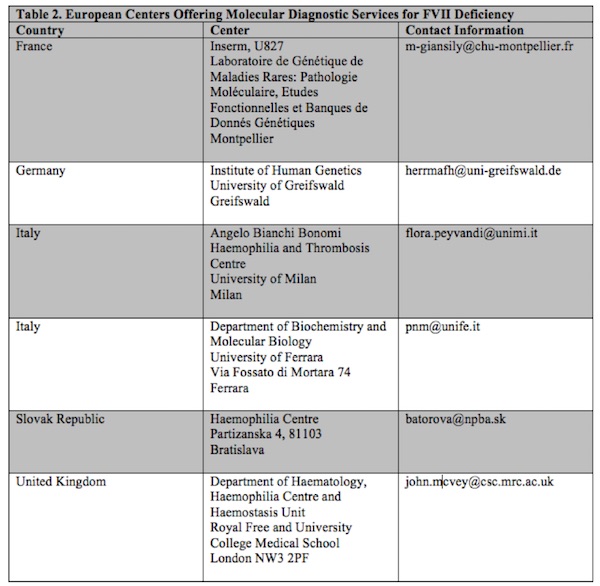
Molecular diagnosis of FVII deficiency is available at the following centers in Europe (Table 2):
Laboratory tests/procedures
Diagnosis of FVII deficiency is straightforward: FVII deficiency is the only explanation for an isolated, prolonged prothrombin ratio (or INR), where the PT is prolonged but the aPTT is normal. The INR prolongation may be moderate (1.5-1.8) to high (> 2.0). Diagnosis is confirmed by the specific FVII assay, possibly carried out with the modern, recombinant thromboplastins that are now available. A thrombin generation assay may also be performed. Genotypic analysis is useful only for clinical studies, or to carry out a prenatal diagnosis.
