
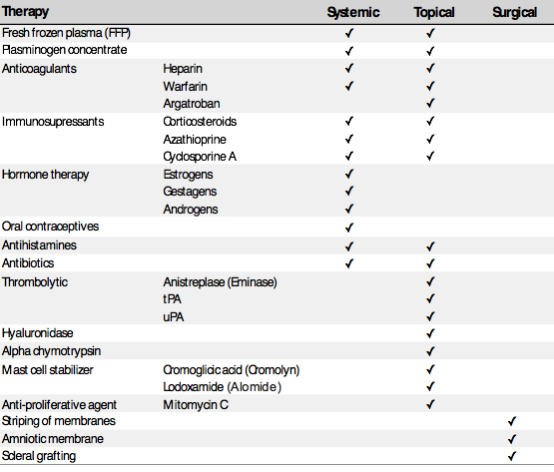
Most of the data on plasminogen deficiency comes from case reports, which limits the ability to draw firm conclusions regarding optimal treatment approaches. Several topical and systemic medications have been utilized to treat clinical symptoms associated with plasminogen deficiency, but agents other than specific plasminogen concentrate replacement therapy are inconsistently effective (Table 1).1,12,19,48 Most non-replacement therapies have targeted inhibition of inflammation or fibrin generation; this approach is reasonable in the absence of specific replacement therapy given the pathophysiology of lesion development with accumulation of fibrin rich tissue often stimulated by inflammation.12
Table 1. Published reports of treatments for plasminogen deficiency
Immunosuppressive agents including steroids, cyclosporine, and azathioprine have been utilized topically or systemically with limited or intermittent success.1 Unfortunately, no consensus has been established to determine the most effective dosing of systemic or topical steroids. Topical cyclosporine emulsions ranging from 0.1 to 2% applied every 2-6 hours seem to reduce the severity and reduce recurrence of ligneous lesions.1
Topical heparin and argatroban have been attempted with some success.29,49, 50 One report described success with systemic warfarin anticoagulation.51
Hormone replacement therapy (HRT) was shown to increase plasminogen levels.52 An increase in plasminogen levels with improvement of ligneous lesions was also reported when oral hormonal therapy was instituted in two women of child-bearing age.53 Stanozolol has also been tried.54 The use of either systemic or topical fresh frozen plasma (FFP) as a source for plasminogen has been associated with some success,55 and in the last few years has gained momentum as a therapy in the absence of plasminogen concentrates.56 IV FFP should be used in the peri-operative settings or in life-threatening situation e.g. airway and lung involvement. The ability to increase plasminogen activity by IV FFP without fluid overload is limited. By convention, pooled plasma contains 1 unit of plasminogen per mL, but individual units may vary. A dose of 10 ml/kg should increase factor activity by ~10% and may provide a clinically sufficient increase in plasminogen activity.
It is important to note that in the absence of plasminogen concentrates, therapy should be based on a combination of modalities to achieve best clinical results, and in fact, most of the reported treatment modalities utilize combinations of agents.29 Data from recent clinical trial utilizing plasminogen concentrates is reported below under research section.
Ligneous conjunctivitis: The following topical therapies have been reported to be effective for ligneous conjunctivitis: Plasminogen ophthalmologic drops,57 FFP, heparin, corticosteroids, cyclosporine, azathioprine, plasminogen activators (e.g. tPA), hyaluronidase, α-chymotrypsin, cromolyn with an antimicrobial, antihistamines, lubricant ointments and artificial tears.1,12,19,48
It is important to keep in mind that although surgical procedures may provide some temporary relief, ligneous lesions quickly regrow without adequate and aggressive perioperative management. Thus, surgical procedures should be reserved to prevent vision impairment or performed only when plasminogen concentrate, either topical or systemic therapy, is utilized.39,58
Recently, in the absence of either topical or systemic plasminogen concentrates, the authors have treated patients with FFP eye drops in combination with commercially available Cyclosporine (0.05%) and short courses of topical steroids and topical antibiotics supplemented with antihistamines or artificial tears when indicated. This approach has resulted in decreased severity of lesions and reduced recurrence (unpublished results). FFP eye drops are prepared by a blood bank utilizing a unit of type-compatible FFP to generate small segmental aliquots of 1 ml each. Random donor is generally preferred. Aliquots remain frozen until use when 0.5 ml of FFP is applied to each eye 4-6 times per day and increased to 12 times per day preoperatively and weaned gradually postoperatively. Cyclosporine is applied 3-5 times daily.
Ligneous gingivitis/periodontitis: Ligneous gingivitis/periodontitis due to plasminogen deficiency is difficult to treat, but the following combination has been used with some success: oral hygiene (dental scaling), root planing and chlorhexidine rinse, systemic antibiotics covering anaerobes, topical steroid rinses, and systemic steroids. Gingivectomy or other periodontal surgical procedures are not reported to be helpful and should generally be avoided given the potential risk of worsening the condition.31,59,60,61,62,63 Systemic therapy utilizing IV plasminogen concentrate has shown to be effective.39
Ligneous lesions of the female reproductive tract: Data are very limited and no topical therapies are available, but oral contraceptives have been proposed.35 A heparin-like preparation has been attempted, but the outcome was not described.36 Minimizing procedures including biopsies is likely the best approach in the absence of effective therapy. The use of IV plasminogen concentrate resulted in significant improvement.39
Hydrocephalus: Congenital hydrocephalus is a known complication in pediatric patients with plasminogen deficiency. Unfortunately, these patients may require multiple shunt revisions due to recurrent shunt occlusion in the absence of effective systemic therapy.43 Ventriculocholecystic shunt procedures have been performed successfully and summarized in a literature review by Demetriades, et al.44
Topical and systemic plasminogen concentrates: Both topical and systemic plasminogen concentrates have been investigated and have demonstrated efficacy.2,64,65,66 Treatment with systemic Lys-plasminogen in a young child with ligneous conjunctivitis was reported in 1998. Ophthalmologic lesions improved and/or resolved when plasminogen activity levels were maintained at 40-50% and lesions were able to be surgically excised without recurrence. Withholding therapy for 48 hours resulted in early lesion recurrence, which resolved following re-initiation of systemic therapy.2 Four subsequent studies demonstrated the efficacy of topical plasminogen ophthalmologic drops in treating ligneous conjunctivitis.57, 64,65,66 Interestingly, one study reported initial use of topical plasmin therapy as ineffective, but subsequent use of topical plasminogen was effective;65 this is likely due to the very short half-life of plasmin and the fact that plasmin doesn’t bind to the deposited fibrous material. A systemic plasminogen concentrate was reported as successful in an infant with ligneous conjunctivitis.2 The current lack of an available regulatory agency-approved efficacious local or systemic plasminogen replacement product represents an important therapeutic gap. Fortunately, two recent clinical trials with promising results have investigated the use human plasma-derived plasminogen concentrates in patients with hypoplasminogemia (see Research section). A phase 2/3 clinical trial with a systemic Glu-plasminogen concentrate has been conducted and has been submitted to regulatory agencies. Licensure of this agent will be a significant advance for the affected population.
